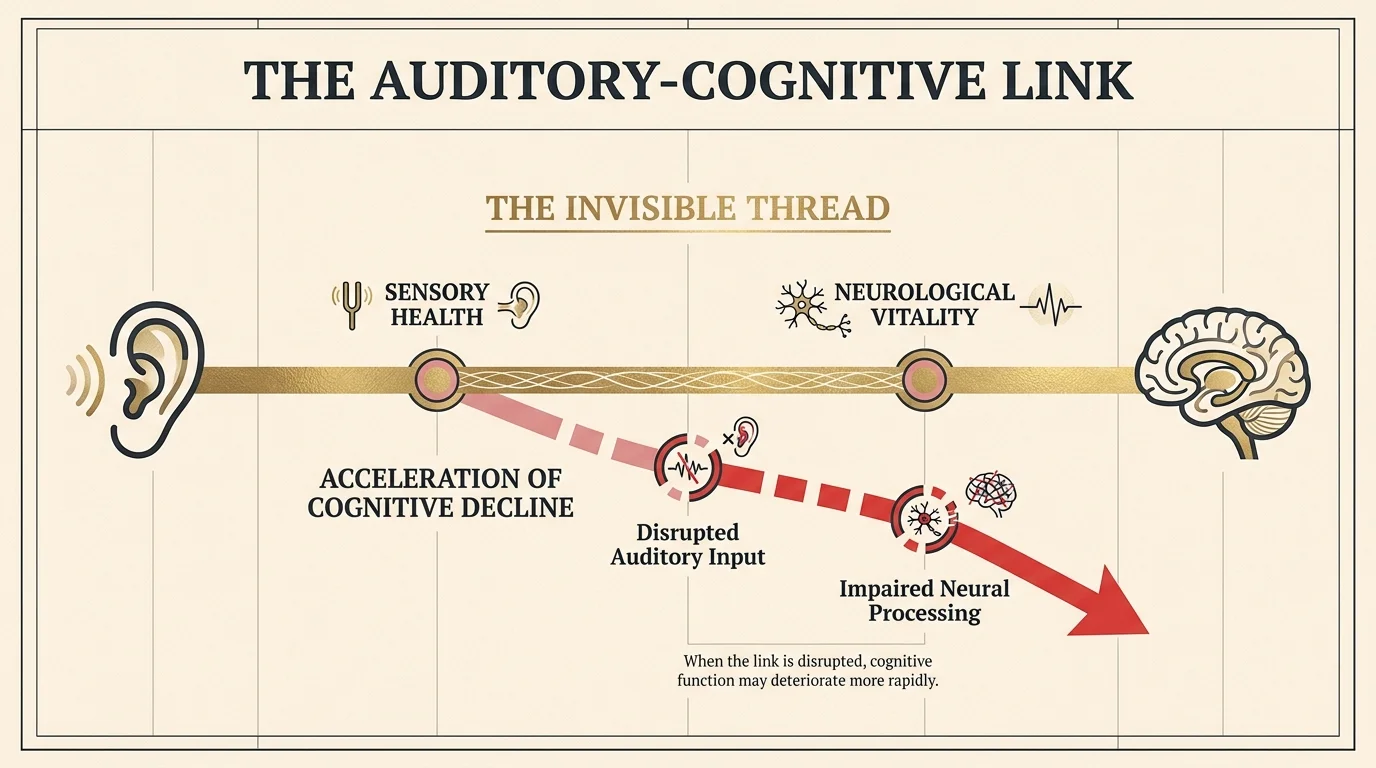
When you sit on the examination table waiting for your physician, you likely run through a familiar mental checklist. You prepare to discuss your blood pressure, review your latest cholesterol panel, and perhaps mention that lingering ache in your lower back. These are the standard benchmarks of a senior medical visit. Yet, as medical science looks deeper into the aging process, researchers are discovering that the most critical conversations you can have with your physician often involve the hidden connections between seemingly unrelated bodily systems. One of the most profound and startling discoveries in recent years is the invisible thread linking your sensory health to your neurological health.
You might assume that asking for checkup tips 60+ simply means requesting adjustments to your medication or securing a referral for a routine colonoscopy. However, true preventative health requires a broader perspective. A comprehensive doctor appointment guide today must address the emerging science of whole-body interconnectivity. Specifically, researchers have uncovered a massive, undeniable link between untreated hearing loss and the acceleration of cognitive decline. Understanding this connection changes everything about how you should approach your healthcare.
If you want to protect your memory, your independence, and your overall vitality, you must update the way you talk to doctor seniors specialists. Rather than passively accepting the tests your physician orders, you need to drive the conversation toward preventative, cross-system monitoring. By understanding the intricate relationship between your ears and your brain, you can utilize the specific questions ask doctor protocols outlined in this guide to transform your next checkup into a powerful strategy session for your long-term cognitive health.
Understanding Age-Related Hearing Loss
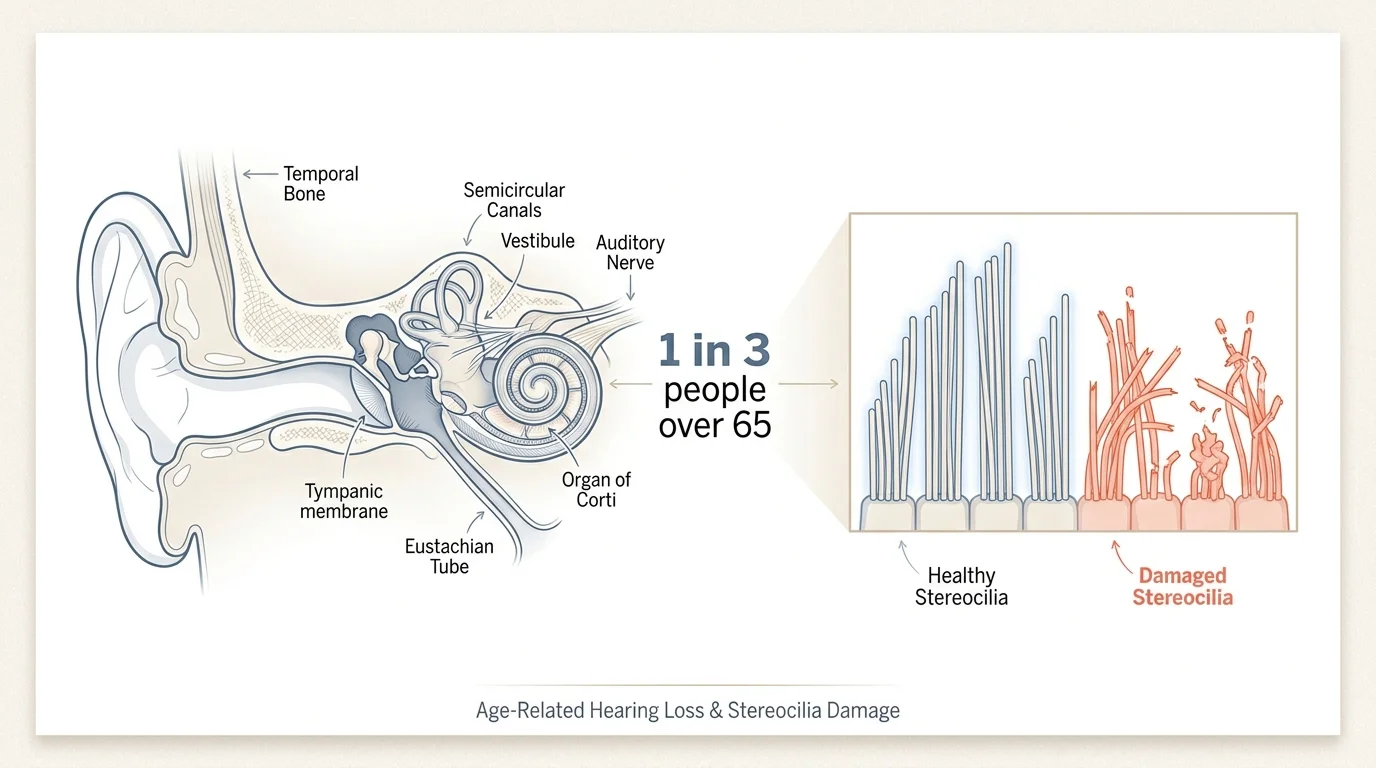
Age-related hearing loss, medically known as presbycusis, is one of the most common conditions affecting older adults. Despite its prevalence, it remains deeply misunderstood and frequently ignored. According to the World Health Organization, nearly one in three people over the age of sixty-five experiences disabling hearing loss. The process rarely happens overnight; it is a slow, insidious fade that gradually filters out the high-frequency sounds of your world. You might first notice that consonants like “s” and “f” blur together, making human speech sound mumbled, or you might find it increasingly difficult to isolate a single voice in a crowded, noisy restaurant.
To grasp why this happens, you must look deep inside your inner ear. Nestled within your temporal bone lies the cochlea, a fluid-filled, snail-shaped structure lined with thousands of microscopic hair cells known as stereocilia. These remarkable cells act as biological microphones. They catch the mechanical vibrations of sound waves and convert them into electrical signals that travel up the auditory nerve to the brain. Over decades of life, exposure to loud noises, environmental toxins, restricted blood flow, and the natural aging process causes these delicate hair cells to bend, break, or die off entirely.
Crucially, human beings cannot regenerate inner ear hair cells. Once a stereocilia perishes, the specific frequency it was responsible for transmitting goes permanently silent. Because the cells responsible for high-frequency sounds sit at the base of the cochlea—where all sound waves enter—they endure the most wear and tear off the bat. This anatomical reality explains why you might hear the low rumble of a truck perfectly well, yet fail to hear the high-pitched chirp of a microwave or the soft voice of a grandchild. When these subtle auditory cues vanish, your brain receives an incomplete puzzle, forcing it to work significantly harder just to navigate a normal conversation.
Understanding the Mechanisms of Cognitive Decline
On the other side of this physiological equation is your brain. Cognitive decline is a broad term that encompasses a range of changes in memory, processing speed, and executive function. It is entirely normal for your brain to undergo slight structural and functional shifts as you age. Your processing speed might slow down a fraction of a second, or you might occasionally struggle to recall a specific noun. However, pathological cognitive decline—the kind that leads to conditions like Alzheimer’s disease and other forms of dementia—involves a much more aggressive deterioration of neural networks.
The human brain is a marvel of neuroplasticity; it possesses an incredible ability to rewire itself, form new synaptic connections, and adapt to changing circumstances. In youth, this neuroplasticity is robust and fast-acting. As you enter your later years, neuroplasticity naturally decelerates. Simultaneously, your brain begins to lose volume. Grey matter, which contains the cell bodies of your neurons, thins out, particularly in the hippocampus and the frontal lobes—the regions most responsible for memory consolidation and complex problem-solving.
Major research institutions, such as the Alzheimer’s Association, note that dementia is driven by a complex interplay of genetic, environmental, and lifestyle factors. In Alzheimer’s disease specifically, toxic proteins like beta-amyloid form plaques between neurons, while tau proteins form tangles inside the cells, ultimately choking off the neuron’s nutrient supply and causing cell death. Even in the absence of Alzheimer’s, microvascular disease—where the tiny blood vessels supplying the brain become stiff and narrow—can starve neurons of vital oxygen and glucose, accelerating cognitive impairment. The health of your brain relies heavily on constant, meaningful stimulation and robust blood flow to maintain its existing neural architecture.
The Surprising Connection: How Your Ears Shape Your Brain
For decades, the medical community viewed hearing loss and cognitive decline as two parallel but completely separate miseries of aging. You went to an audiologist for your ears and a neurologist for your brain. This siloed approach shattered when longitudinal studies—most notably those spearheaded by researchers at the Johns Hopkins Bloomberg School of Public Health—revealed a staggering correlation. Mild hearing loss doubles your risk of developing dementia. Moderate hearing loss triples the risk. Severe, untreated hearing loss makes you five times more likely to develop dementia.
This is not merely a statistical coincidence. Scientists have identified three primary mechanical theories that explain exactly how degrading sensory input physically alters the brain and accelerates cognitive decline.
The Burden of Cognitive Load
The most widely accepted explanation for the hearing-dementia link is the concept of cognitive load. Think of your brain as a computer with a finite amount of random access memory, or RAM. When you have normal hearing, your brain effortlessly decodes the sounds around you, leaving plenty of processing power available to understand the meaning of the conversation, formulate a clever reply, and commit the interaction to your long-term memory.
When you have untreated hearing loss, your brain receives a garbled, degraded audio file. To make sense of the muffled speech, your brain must recruit cognitive resources from other areas—specifically the prefrontal cortex, which is typically reserved for working memory and high-level thinking. By constantly forcing your brain to act as a rigorous audio decoder, you exhaust your mental energy. Your brain uses all its RAM just trying to figure out what was said, leaving zero processing power left over to actually save the memory of the conversation. Over years, this relentless cognitive overload exhausts the brain’s reserves, unmasking dementia symptoms much earlier than they might otherwise appear.
Brain Atrophy and Structural Changes
The second mechanism involves the physical structure of the brain itself. The “use it or lose it” principle applies directly to your neural architecture. When auditory signals from the inner ear decline, the specific areas of the brain responsible for processing sound—primarily the auditory cortex in the temporal lobe—stop receiving their usual stream of electrical stimulation.
Without regular stimulation, the neurons in these regions begin to shrink and die off. Advanced neuroimaging shows that older adults with untreated hearing loss experience an accelerated rate of brain tissue loss compared to those with normal hearing. What makes this brain atrophy particularly dangerous is that the shrinkage does not remain neatly confined to the auditory cortex. The atrophy spreads to adjacent regions, including the areas responsible for memory and spatial orientation. You are quite literally allowing your brain tissue to waste away by starving it of sound.
Social Isolation as a Catalyst
The final mechanism bridging these two conditions is deeply rooted in human behavior. Communication is the bedrock of human connection. When you cannot easily follow a conversation, social interactions transition from being a source of joy to a source of profound exhaustion and embarrassment. You might smile and nod at a dinner party without actually understanding the joke, or you might decline invitations to loud family gatherings altogether to avoid the frustration.
This gradual withdrawal leads to severe social isolation. Extensive research demonstrates that chronic loneliness and social isolation are toxic to the human brain. Social engagement provides a rigorous, multi-faceted cognitive workout. It requires active listening, emotional processing, and rapid verbal reasoning. When you withdraw socially due to hearing loss, you strip your brain of this vital daily exercise, allowing cognitive decline to accelerate unimpeded in the silence of isolation.

What This Means for Your Health
Understanding this biological chain reaction fundamentally shifts how you must view preventative medicine. Hearing loss is not a benign, inevitable annoyance of getting older; it is a major, modifiable risk factor for dementia. The Lancet Commission, a highly respected international body of researchers, recently declared that addressing mid-life and late-life hearing loss is one of the single most effective things a person can do to prevent or delay the onset of dementia.
This revelation should empower you. While you cannot change your genetics or completely halt the passage of time, you have absolute control over how you manage your sensory health. Treating hearing loss is no longer just about turning up the volume on your television. It is a vital neurological intervention. By ensuring your brain receives crisp, clear auditory signals, you reduce your cognitive load, prevent sensory-deprivation brain atrophy, and keep yourself socially engaged. All of these factors build a robust cognitive reserve that can physically protect your brain against the pathological markers of dementia. This science demands a proactive, aggressive approach during your regular medical evaluations.
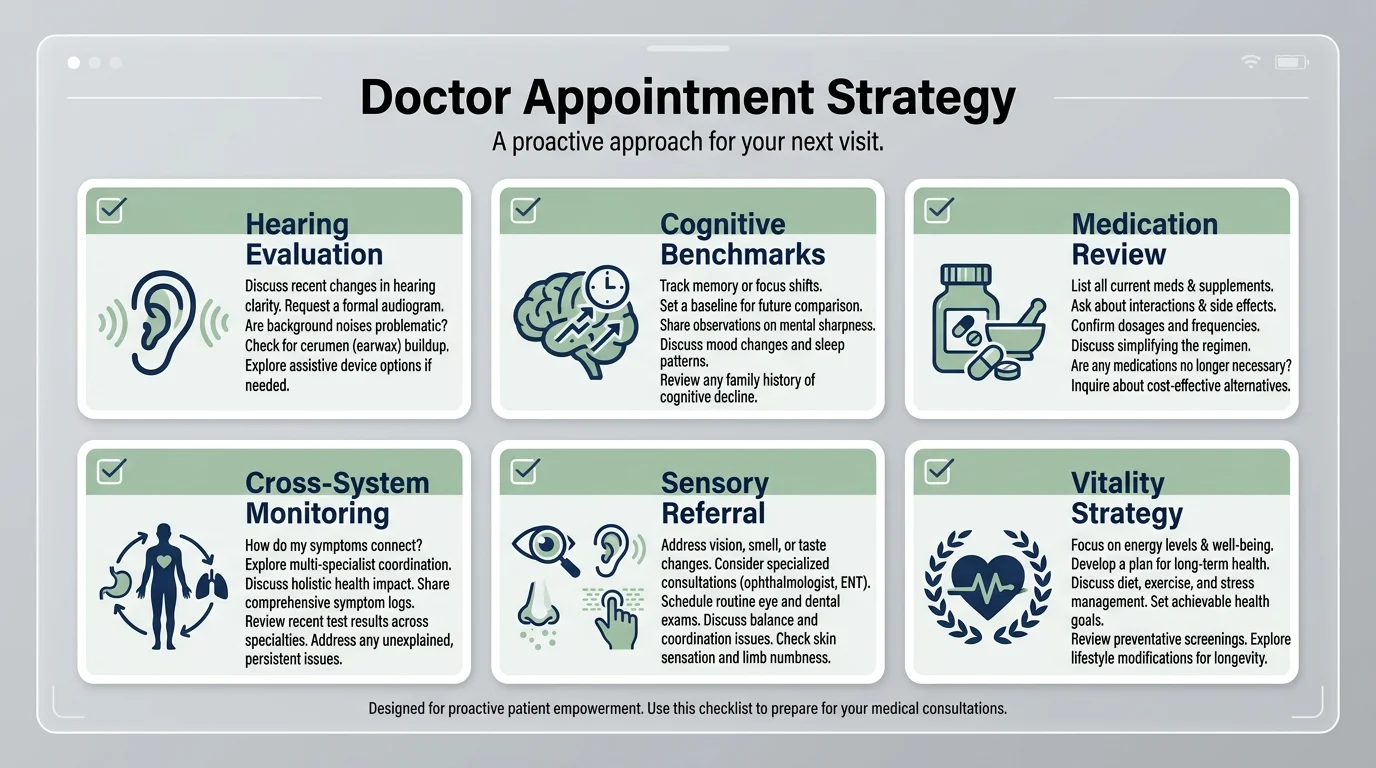
Proactive Measures You Can Take: The 6 Questions to Ask
Knowing the science is only the first half of the battle; the second half is leveraging that knowledge in the examination room. Primary care physicians operate under severe time constraints, and they often focus strictly on immediate, life-threatening metrics like blood sugar and cholesterol. If you do not bring up your sensory and cognitive health, they likely will not either. To bridge the gap between emerging science and everyday clinical practice, you must come prepared. Here are the specific, actionable questions you need to ask your doctor to protect your whole-body health.
Question 1: When should I schedule a comprehensive baseline audiogram?
Do not wait for your doctor to pull out an otoscope and whisper in your ear during a physical. The crude hearing screenings performed in a standard primary care office are highly inaccurate and routinely miss high-frequency hearing loss. You need to ask for a referral to a certified audiologist for a comprehensive baseline audiogram. This test takes place in a soundproof booth and measures exactly which frequencies you can hear and how well your brain understands speech in background noise. Establishing this baseline while you are relatively young—ideally in your early sixties—gives your medical team a concrete standard against which to measure future decline. If you catch the subtle shifts early, you can intervene before cognitive load begins to exhaust your brain.
Question 2: Are any of my current medications contributing to cognitive fog or ototoxicity?
Many older adults take a daily cocktail of prescription drugs to manage chronic conditions. What most patients do not realize is that hundreds of common medications are ototoxic, meaning they contain chemicals that can temporarily or permanently damage the delicate hair cells in the inner ear. Certain heavy-duty antibiotics, loop diuretics used for heart failure, and high doses of nonsteroidal anti-inflammatory drugs can all compromise your hearing. Furthermore, many anticholinergic medications—such as over-the-counter sleep aids, allergy pills, and certain antidepressants—block a neurotransmitter called acetylcholine, directly causing cognitive fog and memory issues. Ask your doctor to conduct a thorough medication review to identify any drugs that might be silently harming your ears or dulling your mind, and inquire about safer, alternative therapies.
Question 3: Based on my cardiovascular health, what is my specific risk for accelerated brain aging?
The health of your vascular system dictates the health of both your inner ear and your brain. The cochlea relies on a heavily vascularized tissue bed called the stria vascularis to maintain the electrical charge necessary for hearing. Similarly, your brain relies on a vast network of capillaries to receive a steady flow of oxygen. If your doctor tells you that you have hypertension, high cholesterol, or early-stage diabetes, you must ask them to explain how these conditions are impacting your microvascular health. High blood pressure acts like a power washer against the delicate linings of your smallest blood vessels, leading to micro-strokes in the brain and oxygen starvation in the inner ear. Treating your heart health is directly treating your brain and sensory health.
Question 4: What cognitive baselines should we establish today to monitor future changes?
Just as you measure your blood pressure to catch hypertension before a heart attack, you should measure your cognitive function before severe memory loss sets in. Ask your doctor to administer a brief, standardized cognitive assessment during your visit, such as the Mini-Mental State Examination or the Montreal Cognitive Assessment. These simple, ten-minute tests evaluate your memory, attention, language, and visuospatial skills. Having a documented baseline in your medical file is invaluable. If you or your family notice subtle behavioral changes three years down the line, your physician can administer the test again and compare the results objectively, removing the guesswork and allowing for immediate, targeted interventions if true cognitive decline is beginning.
Question 5: Can you recommend a local specialist or program for auditory rehabilitation if I need hearing aids?
If your audiogram reveals that you do, in fact, have age-related hearing loss, acquiring a hearing aid is only step one. Ask your primary care physician to guide you toward comprehensive auditory rehabilitation. When you first put on a hearing aid, your brain is suddenly flooded with high-frequency sounds it has not processed in years—the hum of the refrigerator, the rustle of newspaper, the clicking of shoes on a hard floor. This sudden influx can be incredibly overwhelming and is the primary reason many seniors relegate their expensive hearing aids to the bedside drawer. Auditory rehabilitation involves working with an audiologist to slowly train your brain to filter and process these sounds again. Asking this question ensures your doctor treats your hearing loss as a neurological rehabilitation project rather than a simple retail transaction.
Question 6: How does my family history specifically alter the preventative screening timeline we should follow?
While broad medical guidelines dictate that colonoscopies happen at forty-five and bone density scans at sixty-five, your personal preventative timeline should be uniquely tailored to your genetics. If you have a parent who developed Alzheimer’s disease in their late seventies, or a sibling who required profound hearing assistance early in life, your doctor needs to know. Ask them to overlay your family history onto standard screening guidelines. A strong family history of neurodegenerative disease should prompt your physician to monitor your vascular health, your auditory acuity, and your cognitive baselines far more aggressively and far earlier than the standard protocols suggest. This question transforms you from a generic patient into a personalized case study.
The Future of Research
The scientific community is aggressively pursuing the therapeutic implications of the hearing-dementia link. One of the most critical endeavors in this space is the Aging and Cognitive Health Evaluation in Elders trial, funded by the National Institutes of Health. This groundbreaking research explicitly investigates whether providing older adults with best-practice hearing intervention—including hearing aids and counseling—can physically slow the rate of cognitive decline compared to a control group receiving general health education. Early data strongly suggests that treating hearing loss in individuals who are at high risk for cognitive decline results in a remarkably slower rate of neurological aging. As researchers continue to map out exactly how auditory stimulation preserves brain volume, we will likely see sensory rehabilitation become a primary pillar of global dementia prevention protocols.
Frequently Asked Questions
Does wearing a hearing aid reverse cognitive decline?
While a hearing aid cannot reverse established, pathological dementia like advanced Alzheimer’s disease, it can dramatically improve symptoms of cognitive fog that are caused by cognitive load. When you use a hearing aid, you free up your brain’s processing power, which instantly improves your working memory and attention span. Long-term use of hearing aids has been shown to slow the rate of brain atrophy, effectively putting the brakes on future decline, even if it cannot undo past structural damage.
How often should I get my hearing checked after turning sixty?
Once you turn sixty, you should view a hearing test with the same necessity as your annual bloodwork. You should receive a comprehensive audiogram from a certified audiologist every two to three years. If you already wear hearing aids, or if you have a history of working in noisy environments, you should have your hearing evaluated annually to ensure your devices are perfectly calibrated to your current auditory needs.
Is it normal to feel overwhelmed when talking to my doctor?
Yes, the medical environment is inherently stressful, and appointment times are exceedingly brief. To combat this anxiety, bring a written copy of these six questions with you to the clinic. Do not hesitate to take physical notes while the doctor speaks, or ask if you can record the conversation on your smartphone to review later. Bringing a trusted family member or advocate to act as a second set of ears can also drastically reduce your stress and ensure all your questions are addressed comprehensively.
Can diet and exercise protect my hearing and brain at the same time?
Absolutely. Because both your inner ear and your brain are highly dependent on robust blood flow, any lifestyle choice that improves cardiovascular health will benefit both systems. A diet rich in omega-3 fatty acids, antioxidants, and leafy greens—such as the Mediterranean diet—reduces systemic inflammation and protects the lining of your blood vessels. Regular, moderate aerobic exercise increases the volume of blood pumping through your microvasculature, delivering vital nutrients to your stereocilia and your cortical neurons simultaneously.
Why do doctors rarely bring up hearing loss during routine exams?
Primary care physicians manage an overwhelming number of acute and chronic conditions in highly compressed appointment windows. Hearing loss is entirely invisible, causes no physical pain, and progresses so slowly that patients rarely complain about it unprompted. Furthermore, the historical separation between general medicine and audiology means many general practitioners simply lack the specialized equipment and training to conduct thorough auditory evaluations. This is why you must take the initiative to introduce the topic.
Taking Charge of Your Health Journey
The aging process is not a series of isolated system failures; it is a profoundly interconnected journey. Your ears listen, but it is your brain that truly hears. By recognizing that untreated sensory degradation is a direct threat to your memory, your processing speed, and your social vitality, you can fundamentally alter the trajectory of your aging. When you step into the doctor’s office equipped with the right questions, you stop being a passive recipient of standard care. You become the chief executive of your own wellness. Demand comprehensive baselines, question your medications, and insist on tracking the subtle shifts in your sensory and cognitive health. Your brain requires a rich, loud, and vibrant world to thrive—do not let the silence steal your mind.
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult with your physician or other qualified healthcare provider regarding any medical condition or treatment plan.





